Integrated Neglected Tropical Disease (NTD) Control: The Early Years

Peter J Hotez and the Global Network for Neglected Tropical Diseases discuss integrated control measures for NTDs.
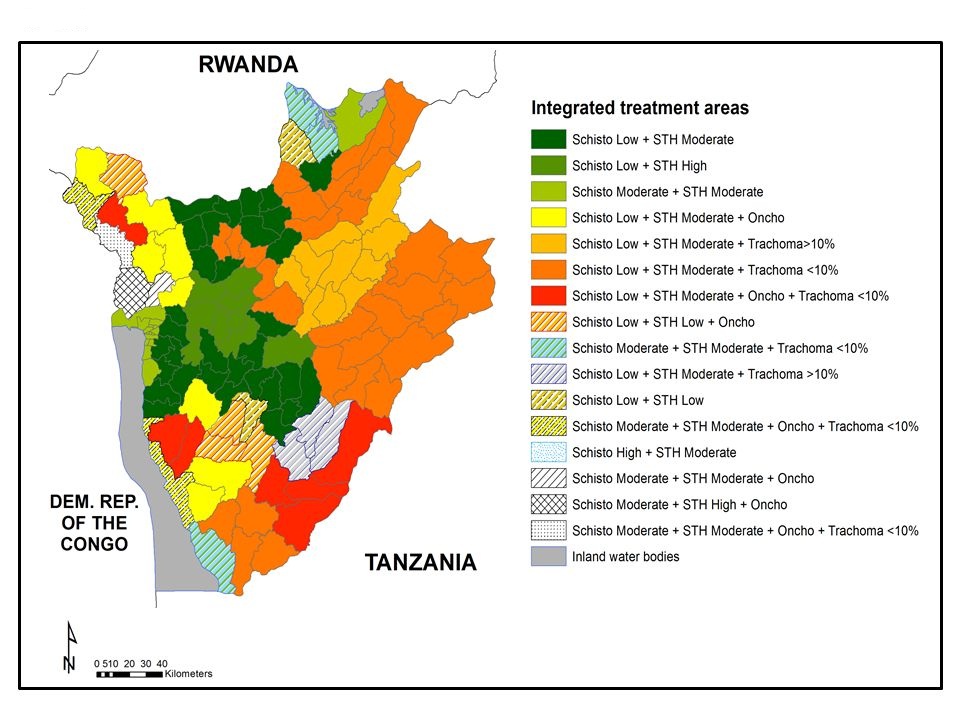
Ndayishimiye et al.
Among the unusual and striking aspects of global integrated NTD control and elimination activities was the exceedingly quick timeline between the time when the concept of integrating NTDs was first proposed and when implementation was initiated. The intellectual framework for a public policy for integrated mass drug administration campaigns that targeted the seven major NTDs simultaneously – ascariasis, trichuriasis, hookworm infection, schistosomiasis, lymphatic filariasis (LF), onchocerciasis, and trachoma – entered the biomedical literature in 2005. Within months a public policy was launched, and expanded implementation of this approach begun.
This month PLOS Neglected Tropical Diseases published a detailed account of a four-year (2007-2011)-long integrated NTD program conducted in the nation of Burundi, a small, densely populated, and landlocked East African nation. When the program began, Burundi had only recently emerged from more than a decade of civil conflict, yet the nation was one of the first few to employ integrated mass drug administration campaigns. The project was launched through private support from the Legatum investment group channeled through the international philanthropy expert, Geneva Global, and ultimately the Global Network for Neglected Tropical Diseases (known previously as the GNNTDC or Global Network for NTD Control) for financial management. SCI (Schistosomiasis Control Initiative) and CBM served as technical implementation advisors to the Ministry of Health (MoH) of Burundi. Together with a parallel program in Rwanda, these two projects established proof-of-principle for successful private financial investments in NTD control, which ultimately led to the establishment of The END Fund.
There are several notable features to the Burundi project. It was one of the first to map NTD endemicity by commune across the nation, and thus could employ algorithms shaped and developed by the World Health Organization (WHO) to decide on the specific NTD drug combinations to be utilized. The four-year project was also highly innovative in that it adapted to the specific needs and requirements for the existing health system in Burundi. For example, when necessary the Burundi MoH used mobile clinics to reach people in remote areas. They integrated vertical programs that were already in place for malaria and onchocerciasis (African Programme for Onchocerciasis Control) with new programs for the other NTDs, which included first-time mass treatments for soil transmitted helminths and schistosomiasis. Integration occurred not only across the different diseases but also across sectors including those committed to maternal and child health and the Expanded Program on Immunization (EPI). The consortium brought on new partners such as UNICEF and leveraged each partner’s strength in order to achieve goals that targeted the NTDs. Moreover, while the Burundi MoH followed WHO guidelines whenever possible in order to implement NTD control, they were also not afraid to make country-specific decisions to reach and treat affected populations.
As for the sustainability of the project, the Burundi’s NTD program continues to leverage private support through active MoH leadership. The good news is that during the four-year period ending in 2011 many of the essential NTD medicines had to be purchased whereas today all of the medicines are being donated free-of-charge.
A clear message is that with modest financial support and technical assistance, the Burundi MoH demonstrated clear ownership and was resolute in solving its own NTD problem. It is especially encouraging to see this happen in the context of Burundi as a post-conflict country: Its NTD program began only two years following the end of a 12-year-long horrific civil war.
In the coming years it will be important to evaluate the long-term effects of integrated NTD control, particularly for its potential to eliminate trachoma, and possibly other NTDs. We certainly agree with the closing recommendations of the authors that a “decentralized routine surveillance system” for detection, management, and follow up care should be structured within its health system, and with a sustained financial commitment from the MoH. We also applaud the Government of Burundi for including NTDs in their 2012 poverty reduction strategy, but emphasize the importance of going beyond the current wording that emphasizes the preparation and review of strategic plans in order to ensure the country uses general development/poverty reduction funds in its actual NTD mass drug administration campaigns.
The authors are with the Global Network for Neglected Tropical Diseases and the Sabin Vaccine Institute. Peter Hotez MD PhD is also the Co-Editor-in-Chief of PLOS NTDs and Dean of the National School of Tropical Medicine at Baylor College of Medicine.
COI Disclosure: The Global Network for NTDs assisted in the financial management and support of the Burundi project described here.