If we are serious about ending TB, we must put quality on the agenda: PLOS Medicine 15th Anniversary

To help celebrate 15 years of PLOS Medicine, Academic Editor Madhukar Pai discusses the advancement of cascades of care in tuberculosis, focusing on a number of contributions in PLOS Medicine since 2016.
Good health is a function of the utilization of healthcare services and the quality of healthcare. In the field of global health, there is growing awareness of the need to go beyond coverage of services and improve the quality of care.
According to a recent report entitled High-quality health systems (HQSS) in the Sustainable Development Goals era, more than 8 million people per year in low and middle-income countries (LMICs) die from conditions that should be treatable by the health system. Sixty-percent of deaths from conditions amenable to health care are due to poor-quality care, whereas the remaining deaths result from non-utilisation of the health system.
Tuberculosis (TB) is the leading infectious killer of humans. TB affects over 10 million people and kills 1.6 million people every year. TB primarily affects poorer sections of the society in low- and middle-income countries.
The HQSS report provides a detailed analysis on TB deaths. Of the 946,003 TB deaths amenable to healthcare, the report estimates that 469,956 (50%) are due to poor quality TB care. The remaining 476,047 deaths are due to non-utilisation of healthcare services.
The fact that 50% of TB patients are dying despite seeking medical care is a sad reflection on the current state of health system performance. How is it acceptable that we cannot save patients with a curable, bacterial infection for which we have policies, tools and technologies?
High-quality care for TB involves early and accurate diagnosis, including drug-susceptibility testing. Diagnosis should be followed by rapid initiation of the correct drug regimen, patient support, and management of relevant comorbidities (e.g. HIV, diabetes). The International Standards of TB Care set out the expectations for quality TB Care.
Sadly, multiple studies show that TB care in many settings does not meet the standards (please see this online lecture on this topic).
Why is the quality of TB care suboptimal? Vital clues are to be found in analyses of cascades of care. This method, widely used to monitor the HIV epidemic, is a model for evaluating patient retention across sequential stages of care required to achieve a successful treatment outcome.
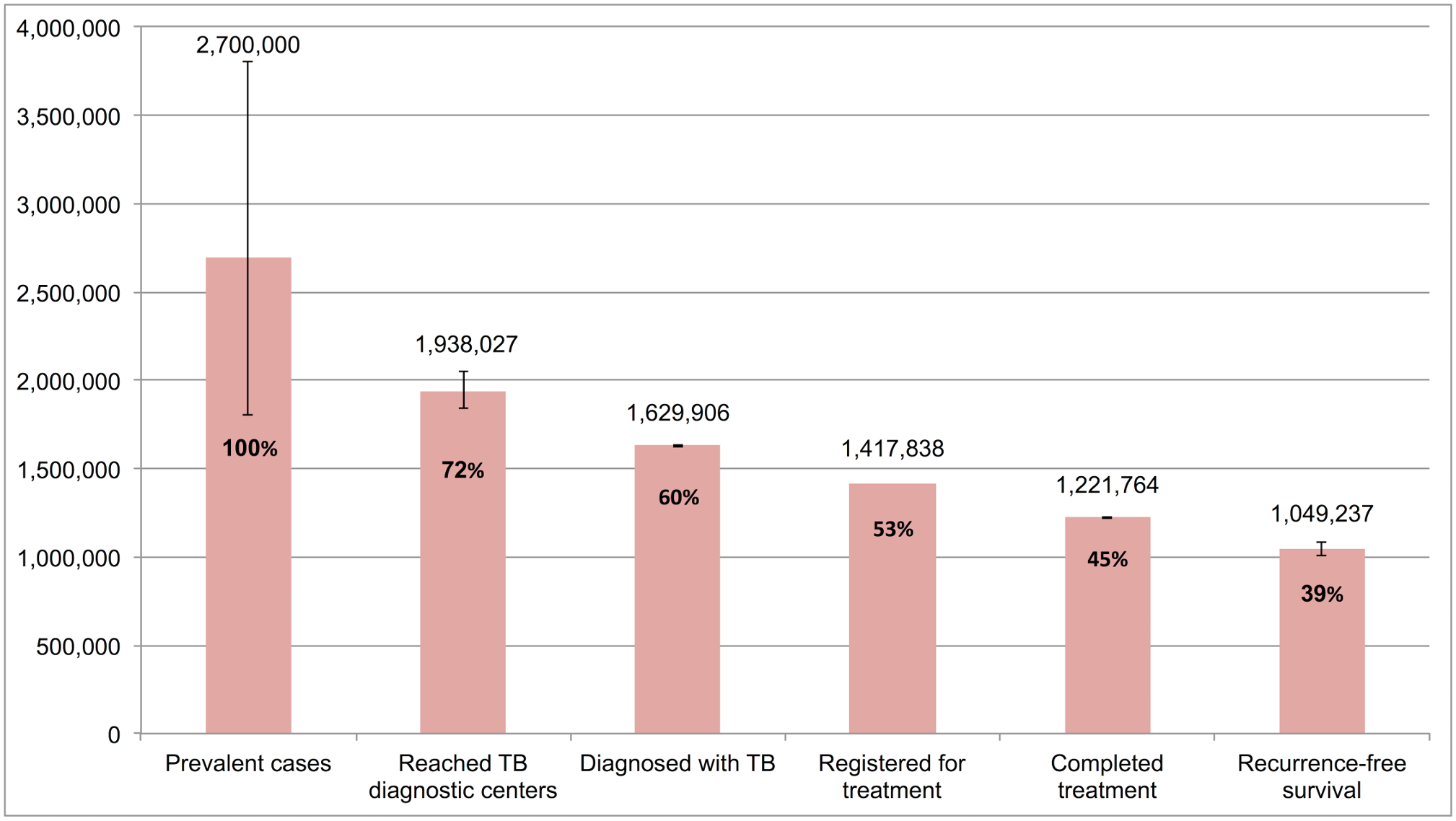
One of the first national TB care cascades was published by Subbaraman and colleagues in PLOS Medicine in 2016. The figure below, from this paper, is the cascade of care for all TB patients in the Indian public sector. Only about 60% of the patients were even diagnosed, and only about 40% reached the finish line (i.e. treatment completion and survival without recurrence).
Similar cascades of care have been published with data from other countries (e.g. South Africa, 30 high-burden countries), for other forms of TB (e.g. latent TB infection), as well as for children. The results are strikingly consistent – across countries, all forms of TB, and risk groups, the cascades of TB care are leaky. Too many people are falling through the cracks.
Further confirmation of low-quality care comes from a novel design that uses mystery clients (standardized patients). Standardised patients (SPs) are people recruited from the local community to present the same case to multiple providers in a blinded fashion. It is increasingly used to measure the quality of care in low-income and middle-income countries.
SP patient studies in 4 countries (India, Kenya, China and South Africa) confirm gaps in cascades of care, and show poor quality of care in both public and private sectors, with private sector faring worse. Across these studies, only about a third of simulated patients with presumed TB were managed correctly at the primary care level.
In a recent PLOS Medicine article, Kwan and colleagues published the world’s largest simulated patient study on quality of TB care in India. The study conducted a total of 2,652 incognito simulated patient visits among 1,203 health facilities in two cities. Only 35% of interactions resulted in correct management during a one-time visit to a private healthcare provider.
A similar simulated patient study in China by Sylvia and colleagues, also published in PLOS Medicine, showed significant quality deficits among village clinics and township health centers in the management of a classic case of presumptive TB.
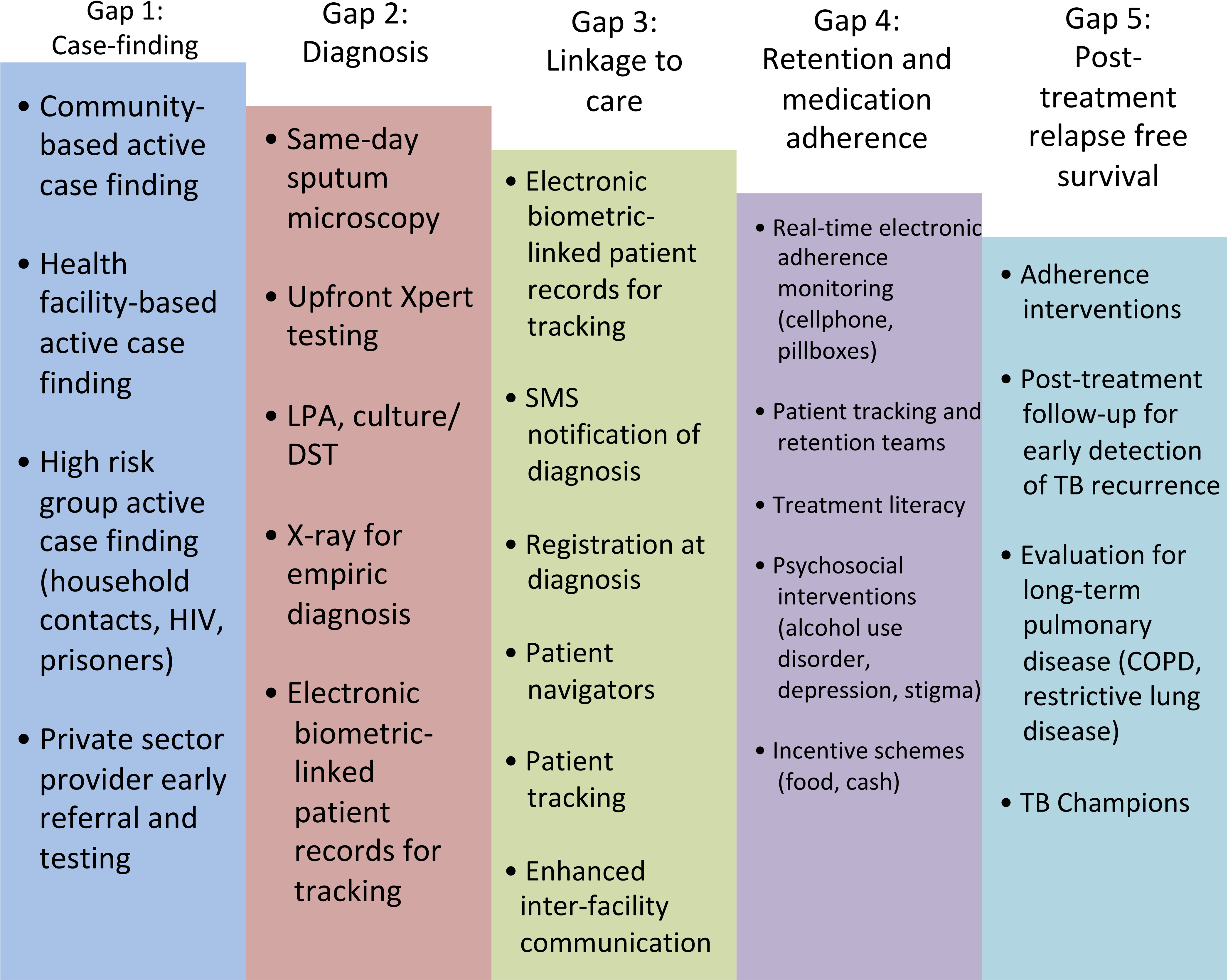
Given the widespread gaps in quality of TB care, it is not shocking that TB is now the number one ranked killer of humans. To change this, we need nothing short of a quality revolution. The TB field urgently needs to adopt and implement the science of quality improvement (QI). This requires all countries to routinely measure cascades of care and use data to identify areas for QI. In a 2019 paper in PLOS Medicine, Subbaraman and colleagues provide a ‘how to’ guide for constructing cascades of care, and for identifying major quality gaps (graphic below).
In addition, Agins and colleagues have provided a nice framework for countries to adapt, if they intend to implement QI for TB. They argue for shifting the focus from “what is wrong” to “how to improve quality.” QI will require National TB Programmes to change the way they organise, use data, implement, and respond to the needs and preferences of people with TB and at-risk communities.
But QI alone is not sufficient, since, as emphasized by the Lancet Commission on Tuberculosis, even the foundations of TB care are weak. Countries need to invest adequate funds to control TB, and make sure TB services are of high quality and patient-centric. In short, if we are serious about ending TB, we must put quality on the agenda, in addition to expanding coverage of critical interventions.
Further reading: The Journal of Clinical Tuberculosis has published an open access series on quality of TB care that can be accessed freely.
 Madhukar Pai is a Canada Research Chair of Epidemiology & Global Health at McGill University, Montreal, where he serves as Director of Global Health, and Director of the McGill International Tuberculosis Centre. His research is mainly focused on improving the diagnosis and treatment of tuberculosis in low and middle income countries. He serves as an editor of the PLOS Tuberculosis Channel, and is on the editorial boards of PLOS ONE and PLOS Medicine. Follow him on Twitter @paimadhu.
Madhukar Pai is a Canada Research Chair of Epidemiology & Global Health at McGill University, Montreal, where he serves as Director of Global Health, and Director of the McGill International Tuberculosis Centre. His research is mainly focused on improving the diagnosis and treatment of tuberculosis in low and middle income countries. He serves as an editor of the PLOS Tuberculosis Channel, and is on the editorial boards of PLOS ONE and PLOS Medicine. Follow him on Twitter @paimadhu.
Image Credit: GDJ, and Clker-Free-Vector-Images, Pixabay (CC0)